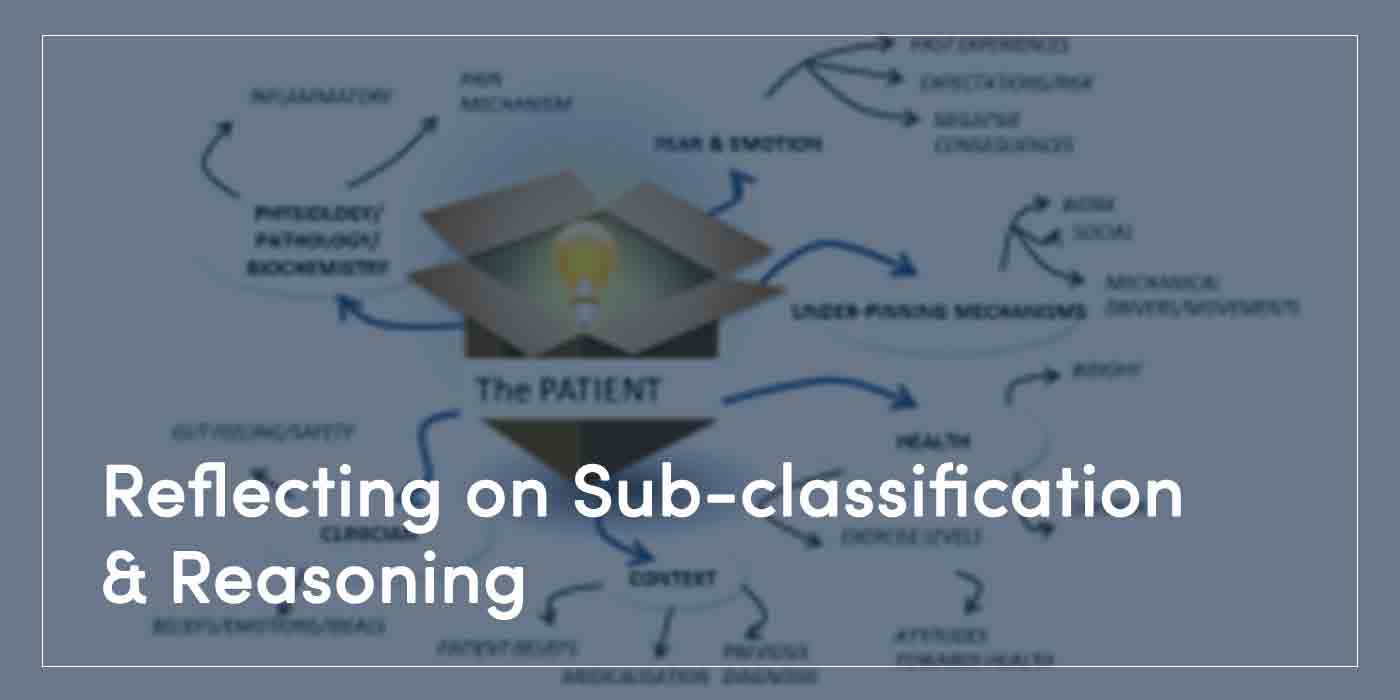
Reflecting on Sub-classification & Reasoning
This week’s Clinical Insight focuses on a topic of discussion at our recent free CPD event, held at AECC University College: the history and utility around sub-classification of low back pain disorders.
Why Sub-Classify Low Back Pain?
It is sometimes helpful to sub-classify low back pain to fit a research narrative; allowing a study to be conducted on a very specific set of constructs in a presentation, which can then be evaluated when it comes to treatment.
Secondly, treatment-based classifications are set up to help set a course of interventions that may have an evidence base behind the algorithm.
In some cases, these are described as clinical prediction rules: a set of observed variables leads to a recommended intervention.
But in reality, the evidence for the benefit of these approaches is not strong (Tagliaferri et al 2022) and only marginal for very specific conditions such as spinal stenosis (Bastos et al 2022).
When looking at the clinical utility of a clinical prediction rules, there again seems to be little use clinically in their application (Walsh et al 2021). Sometimes classifications can be used to help with safety, and in these cases, this can help with good practice.
Red Flags, signs of serious pathologies, will when seen lead to an action, at least of thought and consideration, and possibly referral. Of course, a list of Red Flag questions needs always to be taken into context (Finucane et al 2021), but these are a list of classification questions, and when clustered in context, will inform a decision. But, none of these can really replicate a clinically reasoned approach.
A multi-factorial understanding and appreciation of the factors presented, the influences external and internally, and the changing nature of signs and symptoms.
What Might this Look Like in Low Back Pain?
There are so many factors, and they are all intertwined, that trying to capture that in a process or algorithm is far too challenging.
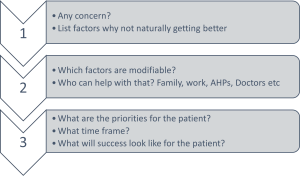
One of our team uses this simple diagram below (Fig. 1) to help with the question “what next?” Essentially starting with why might this problem be continuing, which of those factors are modifiable, who by and in what order.

This then becomes the patient’s own classification – see Fig. 2 and then problem list. This is not presented as an answer, or in any way perfection, but we hope it helps.
References
Bastos, R.M., Moya, C.R., de Vasconcelos, R.A. and Costa, L.O.P., 2022. Treatment-based classification for low back pain: systematic review with meta-analysis. Journal of Manual & Manipulative Therapy, 30(4), pp.207-227.
Tagliaferri, Scott D., Ulrike H. Mitchell, Tobias Saueressig, Patrick J. Owen, Clint T. Miller, and Daniel L. Belavy. “Classification approaches for treating low back pain have small effects that are not clinically meaningful: a systematic review with meta-analysis.” journal of orthopaedic & sports physical therapy 52, no. 2 (2022): 67-84.
Finucane, L.M., Downie, A., Mercer, C., Greenhalgh, S.M., Boissonnault, W.G., Pool-Goudzwaard, A.L., Beneciuk, J.M., Leech, R.L. and Selfe, J., 2020. International framework for red flags for potential serious spinal pathologies. Journal of Orthopaedic & Sports Physical Therapy, 50(7), pp.350-372.
Walsh, M.E., French, H.P., Wallace, E., Madden, S., King, P., Fahey, T. and Galvin, R., 2021. Existing validated clinical prediction rules for predicting response to physiotherapy interventions for musculoskeletal conditions have limited clinical value: A systematic review. Journal of Clinical Epidemiology, 135, pp.90-102.